
Newsletter September 2025
Wrecking ball: Medicaid, Title X cuts will further devastate U.S. reproductive healthcare

When you ban abortion, you harm all reproductive and sexual healthcare. And when you combine that with the U.S.’s recent, massive cuts to healthcare coverage for lower-income folks, you set in motion an out-of-control wrecking ball. We’re about to find out exactly how bad it can get.
The abortion bans in place in 13 U.S. states have already caused considerable harm across U.S. healthcare. Trying to stop people from making one of the most basic of decision about their body, health and life—whether they should carry forward a pregnancy and give birth—is, in and of itself, unacceptable and dangerous. But abortion bans also hurt other aspects of reproductive healthcare, sometimes in unexpected ways.
The so-called “One Big, Beautiful Bill Act” (OBBBA), Trump 2.0’s budget and taxation law adopted on July 4, 2025, will make things even worse. Beginning in 2027, OBBBA will make 15% cuts to Medicaid, the health insurance program for low-income populations, mostly by disqualifying beneficiaries who cannot prove they are working. It’s important to note that the vast majority of able-bodied Medicaid recipients who are able to work are already working. Research shows that only 8 percent of recipients between the ages of 19 and 64 aren’t working, and they are statistically more likely to be poor, older women who left the workforce to care for aging parents or sick children. They will now lose their health coverage.
These and other budget cuts in OBBBA, while made under the guise of “cutting waste, fraud and abuse,” are widely understood to have been made to allow the Trump Administration to extend tax cuts to the wealthy. The non-partisan Congressional Budget Office (CBO) estimates that by 2034, the highest 10% of earners will see incomes rise by 2.7% mainly due to tax cuts, while the lowest 10% will see incomes fall by 3.1% mainly due to cuts to programs such as Medicaid and food aid.
The CBO estimates the cuts will amount to $1 trillion less Medicaid funding between 2025-2034, with 11.8 million people kicked off their Medicaid coverage. Moreover, OBBBA lets the Affordable Care Act’s enhanced premium subsidies lapse (these Biden-era subsidies helped many people obtain health insurance in the private markets), which will cause another 4 million people to become uninsured. In addition, sharp cuts to Title X, which funds family planning for low-income and uninsured individuals, will harm nearly a million people. Of course, all of this is made vastly worse because the U.S., unlike all other industrialized countries, doesn't have universal health coverage, aka Medicare for All.
Far from improving people's access, OBBBA will enact the worst regression in reproductive (and non-reproductive) healthcare coverage we’ve ever seen in the U.S., a decision made by the Republican-controlled Congress. And that will harm all of U.S. healthcare, directly and indirectly.
We should all be worried. VERY worried!
Obstetric care
Abortion bans seek to end all abortions. Interestingly, that has not worked in the U.S., where there were MORE abortions in 2023 and 2024 than in 2021, the year before the U.S. Supreme Court revoked the right to abortion. This isn’t the 1960s anymore and wire coat hangers are largely a thing of the past: today, abortion pills can used safely and effectively at home to terminate a pregnancy, and instructions on how to do so are widely available. Today, an estimated 63% of all abortions in the U.S. are carried out with pills, and abortion pills are shipped to every state, even restrictive ones, by the U.S. postal service.
What abortion bans have done quite effectively, however, is to compromise regular obstetric care. That’s right. Even if you WANT to be pregnant, your obstetric care is compromised by the existence of an abortion ban in your state. That’s because when emptying the content of the uterus becomes a criminal act, health personnel are no longer free to act solely in your interest: they have to worry about the law coming down on them. Penalties for health providers in restrictive states are severe: in Idaho, the law calls for up to 5 years in prison and the revocation of one’s medical license, while Texas’ three anti-abortion laws make providing an abortion punishable by imprisonment ranging from two years to life, the revocation of one’s license, a $100,000 fine for each abortion, and a $10,000 bounty payment to anyone who denounces the health care provider.
Evidence shows that abortion bans have forced obstetricians/gynecologists (OB/GYNS) to provide care that doesn’t meet established medical standards. In practice, this has proven true even in cases of severe pregnancy complications or of fetal defects, where the fetus isn’t viable or wouldn’t survive after birth. In those cases, the traditional standard of care recommends performing an abortion as soon as possible, without delay, to prevent dangerous systemic infections and other injuries to the pregnant person. Yet even in those seemingly clear-cut cases, state-level abortion bans have caused health personnel and hospitals to turn pregnant women away or wait before they take action until women become very sick. As a result, women have died in pregnancy and childbirth. And many pregnant persons who survived suffered serious injuries and trauma.

Pregnant women in Texas faced such dire consequences from the state’s abortion bans that in 2023, 20 of them and two doctors sued the state in Zurawski v Texas. They testified about the consequences of abortion bans on their health: days in intensive care on the verge of death, sepsis, high fever, blackened limbs, permanent damage to major organs, infertility, shock and anguish. Simply horrifying. Unfortunately, the Texas Supreme Court rejected their case, ruling that the women had no standing to sue since they were no longer pregnant (!!), and that the medical exception in Texas law (“to save the life of the woman”) was sufficient to guide doctors’ actions, despite clear evidence that the law had instead caused delays and denials of care that had severely harmed these women.
Unsurprisingly, OB/GYNS in abortion ban states report feeling demoralized, anxious and in emotional distress. In a recent qualitative study of 54 OB/GYNS practicing in states that banned abortion after 2022, clinicians reported feeling “muzzled, handcuffed, or straitjacketed” by legal restrictions on abortion services.
At a national level, evidence is mixed on whether abortion bans are inducing OB/GYNS to leave restrictive states or refuse to train there. But in certain states, that trend is clear: A recent study in the medical journal JAMA found that in Idaho, the number of OB/GYNS fell by 35% between August 2022 (when the state’s near total abortion ban came into force) and December 2024. Out of 268 OB/GYN physicians, a whopping 94 left the state or stopped practicing. Obviously, this affects all persons who need gynecological care, and not only pregnant ones. Ovarian cyst? Endometriosis? Cervical lesions? Fibroids? There are far fewer doctors there for you.
Maternal-fetal health specialists—the doctors who deal with premature babies and severe pregnancy complications—were right behind them. Since 2022, Idaho has lost 55% of its high-risk obstetricians, according to a report by the Idaho Physician Well-Being Action Collaborative. That has left the state with less than five of those specialists full-time, the report found.
The result? Three Idaho hospital labor and delivery departments recently closed: Bonner General Health in Sandpoint, Valor Health in Emmett, and most recently, West Valley Medical Center’s Caldwell facility. Pregnant persons now have to travel long distances for prenatal care or to deliver, a phenomenon described as “obstetric deserts” by Idaho Hospital Association CEO Brian Whitlock in an interview in the Washington State Standard. In the same interview, Valor Health CEO Brad Turpen explained that the Emmett hospital had been unable to consistently staff the maternity ward.
Meanwhile, Steele Memorial Medical Center in Salmon, Idaho, the most remote hospital in the lower 48 U.S. states, paused labor and delivery services because it didn’t have a doctor to staff it, Whitlock added. For women who are pregnant and living in one of the counties served by that hospital, "they are now encouraging you to establish a relationship with a doctor 94 miles away or 168 miles away for your prenatal care and for the delivery of that baby," he noted. "In the meantime, if you have an emergency, go to the hospital. They will stabilize you," Whitlock said. "But you likely will be transported 168 miles away to Idaho Falls for the delivery of your baby."
Oh my goodness. 168 miles (270km) while in labor? This is catastrophic.
Now add to this picture the severe Medicaid cuts voted into OBBBA. Across the U.S., a bad situation is about to get much worse. As a result of OBBBA, at least 300 rural hospitals are at risk of closure. According to health news media KFF, “Federal Medicaid spending in rural areas is estimated to decline by $137 billion [over 10 years], more than the $50 billion appropriated for the rural health fund [the compensation fund Congress included in OBBBA to respond to the worries of rural states].”
Approximately 66 million people – about 20% of the U.S. population – live in rural areas, where the poverty rate is higher than in urban centers. Medicaid covers one in four adults in rural areas and plays a large part in financing health care services. In rural communities, Medicaid pays for nearly half of all rural births and one fifth of inpatient (hospital) care (it’s 41% of births across all states combined). Who will pay for these rural births going forward? It’s doubtful state budgets can pick up the difference.
But ultimately, these huge Medicaid cuts will affect everyone in the U.S., rural and urban, by putting tremendous pressure on many hospitals’ bottom line. “These cuts will indirectly harm the rest of the population by raising financial pressure on health facilities,” noted William Dow, professor of health policy and management at UC Berkeley School of Public Health. “More uninsured people implies more unpaid medical bills, which leads to health care price increases for everyone else. Ultimately, health care facilities in low-income areas will have to cut back on services and based on past experience, we can confidently predict that some safety net clinics and hospitals will be forced to close.”

Maternity wards are often the first services to go in these scenarios. Between 2010 and 2022, more than 500 hospitals across the U.S. dropped obstetrics, according to a recent study. The issue is basically financial: hospitals don’t earn enough from labor and delivery to pay for their costs. “While we are concerned about the impact the bill [the Medicaid cuts in OBBBA] will have on all hospital services, we are particularly concerned about its impact on labor and delivery services,” said Richard Roberson, president and CEO of the Mississippi Hospital Association in a recent interview to news service “The 19th” for an article aptly entitled: Pregnant people are running out of places to give birth.
Swell.
Prenatal care
The trends I’ve described above obviously also affect prenatal care. Now add to that the surge of funding for evangelical Christian, anti-abortion “crisis pregnancy centers” that offer so-called “alternatives to abortion.” Crisis pregnancy centers (CPCs) are “nonprofit organizations that present themselves as healthcare clinics while providing counseling explicitly intended to discourage and limit access to abortion.” They are typically run by untrained volunteers (often dressed in white lab coats) and attract unsuspecting patients “by offering free services such as onsite ultrasounds and STI testing; however, their primary purpose is to discourage abortion, often through manipulative and misleading tactics.”
There are at least 2,500 such centers across the U.S., and probably more. In addition to providing misleading information about abortion, CPCs spread lies about “the harms of hormonal contraception” and “inefficacy of condom use,” and promote sexual abstinence as the only means of preventing pregnancy and sexually transmitted infections (STIs). Their activities tends to delay access by pregnant women to genuine prenatal care, sometimes endangering the health of women who experience pregnancy complications (such as ectopic pregnancies).


For years, significant public funding has been funneled to CPCs—funding that could otherwise go to legitimate health and social services: “Fourteen states now have Alternatives to Abortion programs operated by state agencies and receiving state or federal funding, including Arkansas, Florida, Georgia, Indiana, Louisiana, Michigan, Minnesota, Missouri, North Carolina, North Dakota, Ohio, Oklahoma, Pennsylvania, and Texas. These states have poured over $40 million into anti-abortion centers just this year (2021), a steep increase from past years,” according to a 2021 report by group Equality Forward. The report found that states are also increasingly diverting TANF (Temporary Assistance to Needy Families, the joint federal/state welfare program for the most vulnerable women and children) funds to CPCs, without any oversight.
Contraception and other sexual and reproductive health services
The far-right also wants to eliminate contraceptive and other reproductive health services. This sounds counterintuitive given their avowed concern about abortion, but it reveals the true objective behind their crusade: to control women’s fertility and return them to the kitchen, barefoot and pregnant.
During the first Trump Administration, federal health regulations were revised to disqualify family planning clinics that offered abortion services or provided abortion referrals from receiving federal funding for contraceptive services. As a result, over 1,000 clinics lost their federal funding under Title X, the family planning program that is “a critical part of America’s public health safety net, serving as a point-of-entry into care for nearly 195 million people over the program’s more than 50-year history.” (This statement remains, for the moment, on the U.S. Department of Health and Human Services’ (HSS) website). Title X funds contraception information, services and supplies as well as pregnancy testing and STI testing for close to one million low-income and uninsured people. These Trump regulations were reversed by the Biden administration, and many clinics regained their funding. But some had closed shop in the interim.
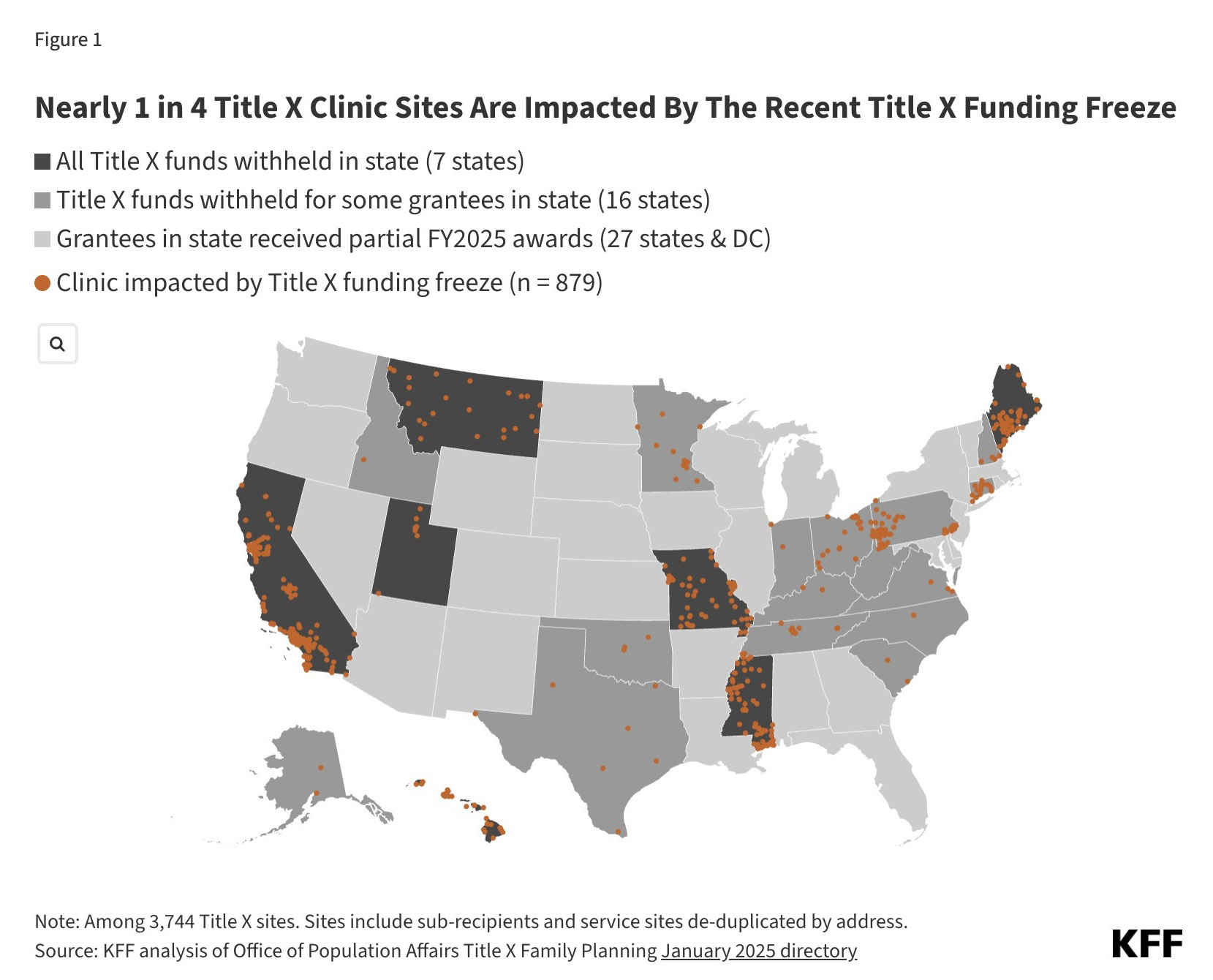
Then, earlier in 2025, HSS struck again, and “withheld” 16 Title X family planning grants amounting to $65.8 million dollars, affecting 870 health facilities across 22 states. HHS invoked “possible violations of …federal civil rights law” to justify these cuts, another example of the administration’s Orwellian campaign of attacks against programs that promote gender and racial equality.
You’ve also no doubt heard of the Republican call to “de-fund” Planned Parenthood, something they pursued unsuccessfully for years. At stake is the ability of Planned Parenthood clinics to receive reimbursement for providing non-abortion health services to people who are insured through Medicaid. The use of federal Medicaid dollars to cover the cost of abortions has been illegal since 1976, so this isn’t about banning federal funding of abortion: it’s about shutting down Planned Parenthood clinics that provide abortions by cutting their revenue stream from all other services.
OBBBA achieved that long elusive goal, essentially barring from Medicaid any nonprofit health clinic that provides abortion and received more than $800,000/year in Medicaid reimbursements in 2023 for non-abortion services such as contraception, STI testing or annual check-ups for cervical cancer. This convoluted funding formula applies almost exclusively to Planned Parenthood affiliates, many of which are larger clinics offering a range of reproductive and sexual health services, along with some primary healthcare services.
Planned Parenthood sued immediately, arguing that it was being singled out for its advocacy for abortion rights, in violation of its First Amendment rights. A nationwide temporary injunction has suspended the application of the budget provision. Yet, faced with the uncertainty of a final ruling (probably by the anti-abortion U.S. Supreme Court), some Planned Parenthood affiliates have stopped serving Medicaid patients or limiting what services they offer them, for fear the federal government could eventually try to claw back the corresponding Medicaid reimbursements. Other affiliates have closed some clinics to deal with the anticipated loss of revenue.
For example, Planned Parenthood Southwest Ohio, one of two affiliates in the state, said in a statement to The Guardian that it was closing two clinics and would no longer accept Medicaid in the remaining two. Planned Parenthood of Greater Ohio, the other affiliate, said that, “while it was accepting Medicaid at its 12 clinics after the injunction, it would not provide intrauterine devices or birth control implants to Medicaid patients – unless they self-pay for the devices and the insertion appointments. These forms of long-acting reversible contraception are some of the most effective, but they are costly and can be hard for low-income patients to access.” Essentially, health providers have concluded, in a most perverse logic created by the Trump administration, that providing poor people with the most expensive services—precisely those services that they most need health insurance for—could eventually bankrupt their clinics.
Should the Medicaid ban for large reproductive health clinics stand, the damage to reproductive health services across the U.S. will be significant. Every year, more than one million patients in 43 states receive Medicaid-covered health care services at Planned Parenthood. Many patients who live in the above-described “obstetric or healthcare deserts” simply can’t go elsewhere for services.
Carrie Cochran-McClain, chief policy officer with the National Rural Health Association, noted in an interview to news service “The 19th” how the gap left behind with each facility closure and health personnel departure affected other aspects of care: “It’s so interconnected. While we’re talking specifically about labor, delivery and pregnancy, it can have an impact more broadly on access to women’s health in rural communities. It’s been a rough couple of years before all of this, so it just feels like it’s a worsening trend in terms of overall access.”
Children’s healthcare
I’d be remiss if I didn’t point out the devastating impact the Medicaid cuts will also have on pediatric care. I’m reminded of the definition of reproductive justice developed in 1994 by African-American feminist activists: “the human right to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.” Massive cuts to healthcare are clearly hostile to that vision.
Currently, Medicaid and CHIP (Children’s Health Insurance Program, child-specific state health insurance programs that usually complement Medicaid) provide health insurance to 47.6% of children in the U.S. Children are generally much healthier than the average population, but when they are sick or disabled, they often require expensive and complex care, particularly to be able to live at home.
While the Medicaid and Affordable Care Act cuts enacted in OBBBA do not target children specifically, there is ample evidence that parents losing their Medicaid or other health insurance will also result in many children losing coverage. For adults, the increased red tape associated with proving that one is engaged in 80 hours a month of paid work or “community engagement” in order to stay on Medicaid will turn away some who were previously eligible, and when that happens, these adults lose contact with the system to maintain or obtain their children’s own healthcare coverage.
And like maternity wards, pediatric wards are vulnerable to being closed when hospitals lose income. Medicaid payments on average cover less than 60% of children’s hospitals’ costs of providing care, with supplemental payments (SDPs, or state directed payments) making up another 20%. (Children’s hospitals make up less than 5% of the nation’s hospitals but account for about 45% of all hospital days for Medicaid-enrolled children). OBBBA will severely cut this essential revenue for pediatric wards and children’s hospitals, particularly in rural areas.
Other cuts will affect children’s health and well-being directly, especially the gutting of SNAP (Supplemental Nutrition Assistance Program) benefits ("food stamps," or vouchers to help the poorest families buy food, currently assisting one in five children in the U.S.). The Center for Budget and Policy Priorities, a non-partisan think tank, estimates that more than 2 million children will see food assistance to their families cut substantially or terminated through 2034, while 3.2 million adults will also lose this support, 800,000 of whom are parents of school-age children. And that’s not all: enrollment in SNAP ensures children’s automatic enrollment in school meal and summer meal programs. This will impact about 420,000 children in an average month.
Disastrous.
The wrecking ball continues to do its damage. Every day, we are pummeled by appalling news as Trump 2.0 becomes more lawless and brazen. It can feel overwhelming. Yet it’s imperative that we keep these shocking facts front and center in our health advocacy and action as we move forward. Attacks on the most vulnerable of us are attacks on us all. There has never been a more urgent time to fight for sexual and reproductive rights, gender and reproductive justice, economic justice and yes! universal health coverage in the U.S. than now.
We shall overcome.
In feminist, reproductive solidarity,
FG